Published in IJCP
January 2023
Review Article
Vascular Calcification in Chronic Kidney Disease
January 13, 2023 | Himanshu Verma, Sham Sunder, Sourabh Sharma
Nephrology
Abstract
Cardiovascular disease (CVD) is the major cause of death in chronic kidney disease (CKD). Of the various risk factors, vascular calcification has only recently come into prominence. CKD is associated with an increased risk of vascular calcification. In routine practice, clinicians usually overlook this finding. Screening for vascular calcification is often missed during first contact with nephrologists. With this article, we would like to reiterate the importance of preventing vascular calcification in early stages of CKD and once it starts appearing, its progression needs to be halted early with individualized treatment. The prevalence, sites of involvement, detection, quantification, pathogenesis, risk factors, clinical manifestations and management options have been discussed.
Keywords: Chronic kidney disease, calcification, cardiovascular disease, metabolic bone disease
The major cause of death in chronic kidney disease (CKD) is cardiovascular morbidity. Though many risk factors are thought to play a role, vascular calcification, especially coronary artery calcification is a risk factor that has only recently come into prominence.1 CKD is associated with an increased risk of calcification which can be in form of solid organ calcification, extraosseous soft tissue calcification or vascular calcification.2 Vascular calcification can appear as intimal calcification, medial calcification, valvular calcification and calcific uremic arteriolopathy.
PREVALENCE
The prevalence of vascular calcification increases with advancing stages of CKD, from 40% in patients with stage 3 CKD, to 80-90% in patients with stage 5 CKD on dialysis (CKD stage 5D).3 In 1997, Goldsmith et al had reported aortoiliac calcification in 39% patients at the onset of dialysis, with increasing risk as age advances. Also, 92% of patients had developed vascular calcification after a mean dialysis vintage of 16 years.4
The presence and extent of vascular calcification are notably higher in patients with CKD as compared to the general population. The prevalence was also higher in comparison to patients with other modifiable and nonmodifiable risk factors of cardiovascular disease (CVD) and normal renal function. Vascular calcification has also been described in young patients on dialysis with childhood-onset CKD, which further supports CKD as an important causative factor.
Sites of Vascular Calcification
CKD patients on dialysis have 30% to 50% risk of developing vascular calcification, the risk further increases in the elderly.5 The blood vessels in the ankle are the earliest and most common site followed by the abdominal aorta, feet, pelvis, hands and wrist.3 In the blood vessel, calcification can involve intima, media and occasionally both. Computed tomography (CT) has demonstrated that 80% to 100% of adult patients on maintenance dialysis develop coronary calcification.6 Intimal calcification is part of advanced atherosclerosis and is associated with cholesterol deposition in atherosclerotic plaques. Intimal calcium deposition is principally associated with myocardial infarction and thrombotic events. It is mostly seen in the elderly. Calcium in the intimal layer may be a marker for plaque vulnerability to rupture and is associated with occlusive disease. However, there are reports that this form of calcification may actually stabilize atherosclerotic plaques and reduce risk of acute plaque rupture. In their opinion, higher load of calcium in vessel walls (intima and media) in uremic subjects may exert a stabilizing effect on arterial plaque lesions by “holding the artery open”, thereby acting in many ways like an adaptive coronary stent.7
Medial calcification (Monckeberg’s sclerosis) may result in palpable arteries, pseudo-hypertension, isolated systolic hypertension, left ventricular hypertrophy and coronary hypoperfusion resulting in significantly adverse cardiovascular outcomes. This is the predominant type of calcification seen in diabetes and CKD.8 Medial calcification is more common in the young, patients on long-term dialysis and those with an elevated calcium-phosphorus product (Ca × P) ratio without conventional atherosclerotic risk factors. Although it is not clear whether Ca × P is a risk factor for vascular calcification. In most cross-sectional analyses of patients with renal failure, vascular calcification has not correlated with Ca × P.9
Vascular calcification can lead to increased pulse pressure, reduced coronary perfusion and abnormal autonomic and endothelial vasomotor functions. Also, there is increased difficulty forming vascular anastomosis (vascular grafts or arteriovenous fistulae) or performing successful coronary artery interventions (angioplasty and coronary artery bypass grafting).10
Detection of Vascular Calcification
Although not clinically useful, the “gold standard” technique for the detection, assessment and quantification of vascular calcification is the histological examination of postmortem arterial specimens. Clinical detection is mostly by plain radiograph, which shows pipe stem (tram line) appearance in case of medial calcification (Fig. 1). CT scanning permits both the detection and quantification of the extent and severity of calcification. Vascular ultrasound can frequently show calcified plaques and calcified media. The use of plain lateral abdominal radiography or echocardiography to detect the presence or absence of vascular or valvular calcification, respectively has been endorsed by Kidney Disease: Improving Global Outcomes (KDIGO).11
Quantification of calcification is done by noninvasive radiology using electron-beam computed tomography (EBCT) and multislice spiral CT.12 This, however, cannot distinguish between intimal and medial calcification.
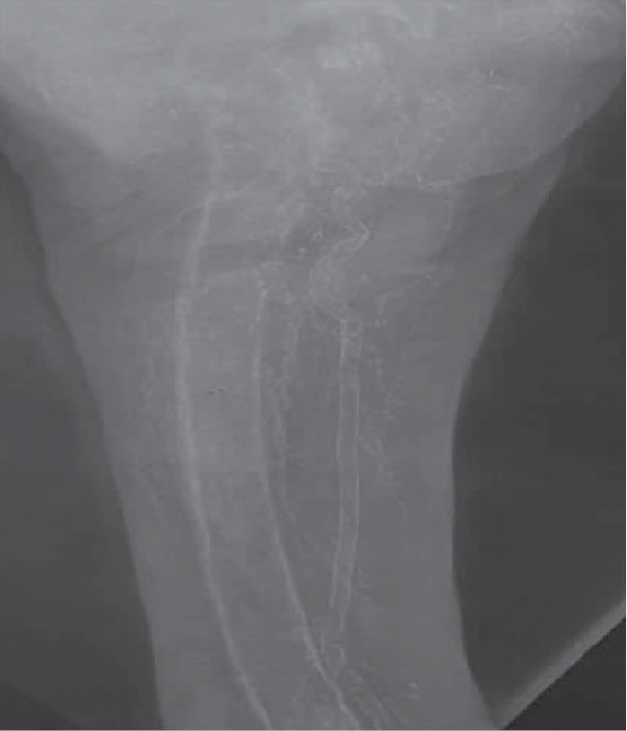
Figure 1. X-ray thigh of a patient of CKD Stage 5D on maintenance hemodialysis with CKD-metabolic bone disease showing pipe stem (tram line) appearance suggestive of medial calcification of femoral artery.
PATHOGENESIS
It was formerly thought that vascular calcification is a passive process caused by elevated phosphate levels and elevated calcium-phosphorus product. It is now felt that vascular calcification is akin to osteogenesis and is an active process involving bone structural proteins and regulators of bone formation with a role for physiological inhibitors of calcification (Fig. 2).13 There are various factors, which could put a patient with CKD at increased risk.14
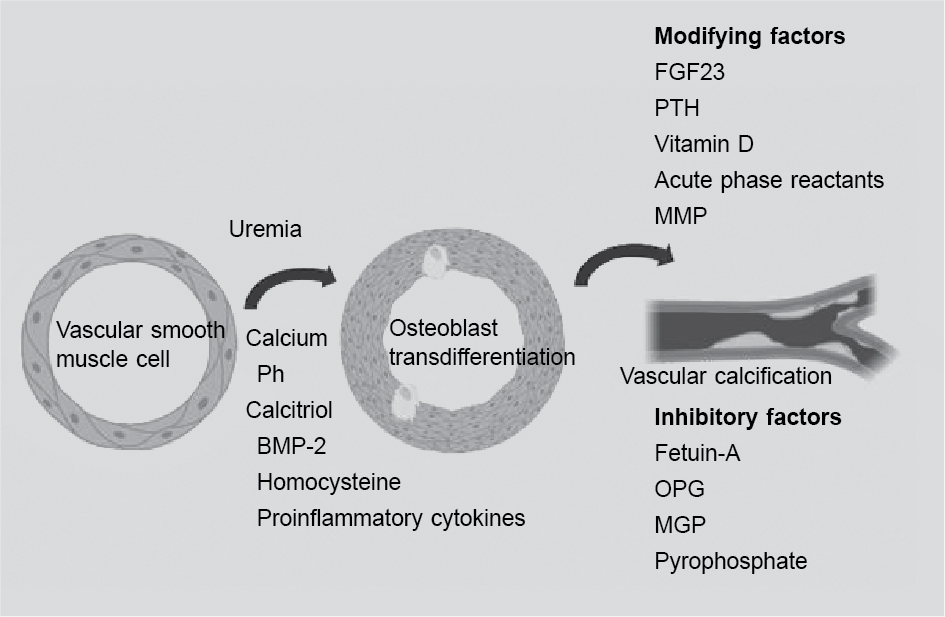
Figure 2. Molecular mechanisms favoring vascular calcification.
Molecular Mechanisms Favoring Vascular Calcification
- Increased amounts of bone-associated proteins: These include osteocalcin, osteopontin, matrix gamma-carboxyglutamic acid (matrix Gla) protein and osteoprotegerin. Runt-related transcription factor 2 (RUNX2) also known as core-binding factor subunit alpha-1 (CBF-α1) are specific transcription factors for osteoblastic differentiation from their mesenchymal precursors and are now thought to play an important role in vascular calcification.15 Elevated phosphorus levels are associated with increased RUNX2 levels.
- Elastin degradation in the blood vessel wall by matrix metalloproteinases favors calcification by inducing over expression of transforming growth factor beta (TGF-β).
- Other mediators of calcification include calcitriol, advanced glycation end products and leptin.
- Loss of inhibitors: Inhibitors of calcification include pyrophosphate, parathyroid hormone (PTH)-related peptide, osteopontin, osteoprotegerin, bone morphogenic protein 7 (BMP 7), matrix Gla protein, fetuin-A, etc. are lost. Low fetuin-A levels are associated with increased risk of cardiac events.16
RISK FACTORS
- Dialysis vintage: More severe calcification is associated with increased dialysis duration.
- Age: Risk is more with increasing age.
- Serum phosphate: A central role for raised plasma phosphate levels has been suggested.17
- Serum calcium: An increased intake of calcium as a phosphate binder may directly enhance coronary arterial calcification. At 1 year, among 200 hemodialysis patients randomly assigned to a noncalcium-based phosphate binder (sevelamer) or a calcium-based phosphate binder, although serum phosphorus control was similar with both agents, sevelamer was associated with a much lower percentage increase of the median absolute calcium scores in both the aorta and coronary arteries.18 As use of sevelamer was associated with a lower calcium level, this suggests a vital role for serum calcium levels in enhancing vascular calcification.
- Diabetes mellitus: Diabetics are at an added risk of vascular calcification irrespective of renal status.
- Magnesium: Several studies have demonstrated presence of two distinct types of calcium phosphates deposits in tissues of patients with chronic kidney failure. Deposits found in periarticular calcifications are carbonate containing apatite, while those found in calcified visceral tissues are either microcrystallites of magnesium whitloekite.19 X-ray diffraction patterns of these two types show tumoral calcification to give apatitie pattern and visceral calcification, an amorphous one. Presence of magnesium may promote formation of this latter type of calcium deposit by disturbing crystallization of apatite and stabilizing amorphous phase as observed in synthetic systems.19
- Active vitamin D: These are used in the treatment of secondary hyperparathyroidism in CKD. Low levels of serum calcitriol are associated with increased risk of calcification.20 Calcitriol suppresses vascular smooth cell proliferation. However, clinically employed doses of vitamin D frequently result in hypercalcemia, which can accelerate extraosseous calcification. The propensity to ectopic/soft tissue calcification is also associated with adynamic bone disease due to excessive vitamin D dosing. Vitamin D therapy, when administered in excess, is a potential vascular toxin, being associated with in vitro phenomena that could predispose to in vivo plaque calcification and atherosclerosis. Thus calcitriol has a dual role in calcification. Vitamin D analogs like paricalcitol, doxercalciferol, etc. which have less propensity for increasing calcium or phosphorus levels may have advantages in preventing calcification.
- Vitamin D deficiency: Vitamin D deficiency appears to contribute in vascular calcification. The pathogenesis include lowered PTH-related peptide levels (which normally inhibit vascular calcification), and suppressed CBF-α1 and bone morphogenic proteins (which enhance the transformation of vascular smooth muscle cells into osteoclast). Thus, both an excess and deficiency of vitamin D can contribute to the vascular calcification via different mechanisms.21
- Inflammation: The chronic inflammatory milieu of uremia may contribute to vascular calcification. A large number of pro-inflammatory or anti-inflammatory substances have been evaluated as possible factors underlying this abnormal milieu. These include osteopontin, osteoprotegerin and fetuin. Osteopontin (a chemoattractant) concentrations in blood and in atherosclerotic plaques are increased in hemodialysis patients compared to age-matched healthy controls, and may correlate with aortic calcification score.22
- Fetuin-A: This is a calcium-binding protein found in serum and produced by the liver. Normal levels of fetuin help clear apoptotic cells, which act as potential nidus for crystal formation in medial arterial calcification by augmenting phagocytosis. Low fetuin levels, which are observed with CKD, other chronic inflammatory states and patients on hemodialysis, are associated with increased vascular calcification, cardiovascular mortality and overall mortality in some studies of dialysis patients.23
- Malnutrition, inflammation and atherosclerosis (MIA) syndrome: It is now felt that the calcium phosphate deposition is not a passive phenomenon but an active one involving increased intracellular phosphate uptake, which can be enhanced in inflammatory states.
- Premature aging-related genes (Klotho and FGF23): Klotho is a transmembrane protein, which acts as a cofactor for fibroblast growth factor (FGF23). Its deficiency is associated with increased risk of calcification.
Other risk factors include increased C-reactive protein (CRP), hyperparathyroidism, parathyroid suppression (adynamic bone disease), decreased serum fibrinogen, hypoalbuminemia, hyperhomocysteinemia and dyslipidemia.
Figure 3 depicts pathogenesis of vascular and soft tissue calcification in CKD patients.
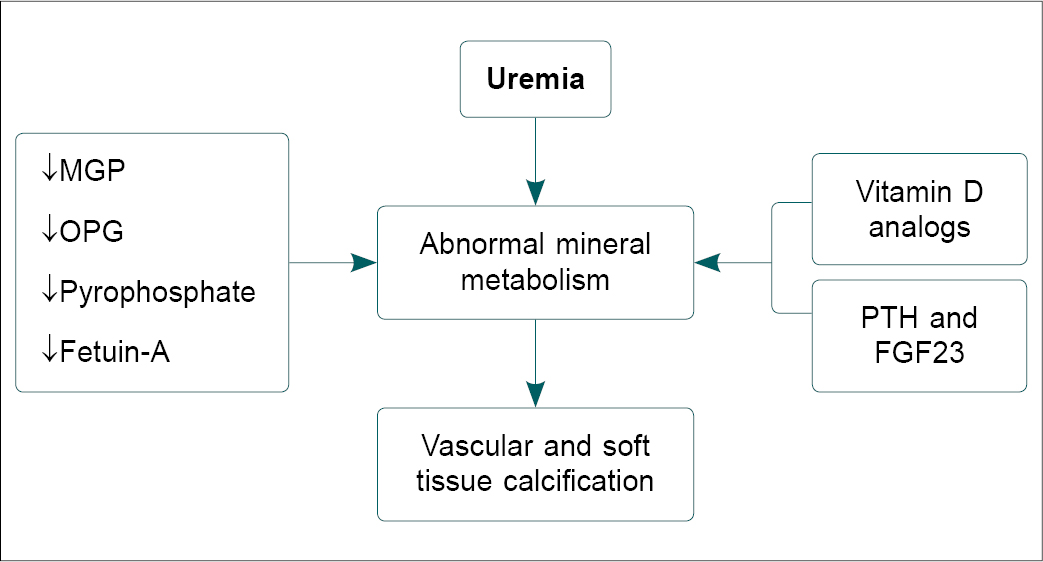
Figure 3. Pathogenesis of vascular and soft tissue calcification in CKD patients.
CLINICAL MANIFESTATIONS
The clinical manifestations may depend on the site of calcium deposition.
- An increase in systolic pressure and a decrease in diastolic pressure with an increased pulse pressure are seen mainly in those with medial calcification.
- Left ventricular hypertrophy
- Angina
- Myocardial infarction and thrombotic events. This is more common in the elderly with risk factors for atherosclerosis. Most patients have predominant intimal calcification.
- Very painful skin lesions and ulcerations following occlusion of small cutaneous arterioles. The typical picture is a mixture of large retiform ulcerations with thick eschar surrounded by violaceous, indurated, tender, retiform plaques. However, the degree of cutaneous and subcutaneous tissue involvement is highly variable and may also be rather limited to livedo reticularis or to a single indurated plaque formation. Compared to those with intimal calcification, patients with medial disease had a longer survival.
PREVENTION AND THERAPEUTIC APPROACHES
There is no evidence-based medicine treatment option available. Treatment is multimodal. The mainstay of therapy in patients with vascular calcification is the normalization of calcium, phosphorus and PTH metabolism. The following are some of the therapeutic options:
- Sevelamer: This drug is a cationic polymer that binds phosphate through ion exchange. lf vascular calcification is found in two or more sites, use of a noncalcium-containing phosphate binder could be considered.24 A new variant of this drug where the hydrochloride moiety is replaced by carbonate is now available. In the “Treat to Goal Study”, 200 patients undergoing maintenance hemodialysis were randomly assigned to sevelamer or calcium-based phosphate binders. At 1 year, although serum phosphate control was similar with both agents, calcium-based phosphate binders were associated with a higher incidence of hypercalcemia (16% vs. 5%) and an increased incidence of low PTH levels.18 A reduction in levels of CRP and uric acid and oxidative stress may contribute to the beneficial effects of sevelamer. Besides, unlike calcium-based phosphate binders, sevelamer also has a bile-acid sequestrant effect, thereby reducing lipid absorption and this could have contributed to the better cardiovascular profile with sevelamer. In the RIND trial, among 129 patients with coronary artery calcium at dialysis initiation, more rapid and more severe increases in calcification were observed with calcium-containing phosphate binders at 12 and 18 months. Those on sevelamer were more likely to show stabilization or regression in coronary artery calcification at 12 months.25 However, despite the possible decrease in vascular calcification with this agent, a well-designed prospective study DCOR, found no difference in cardiovascular mortality or total mortality among hemodialysis patients between sevelamer and a calcium-based phosphate binder.26
- Other noncalcium-containing oral phosphate binders: Lanthanum is an alternative phosphate binder, which does not increase the calcium levels and can be tried to prevent vascular calcification.
- Vitamin D analogs: Drugs like paricalcitol, doxercalciferol may not raise the calcium levels to the same extent as calcitriol.
- Bisphosphonates: Their use has been found to decrease calciphylaxis.27
- Fetuin-A (endogenous inhibitor of calcification)
- Calcimimetics: They seem to be promising agents for treating extraosseous calcifications. Calcimimetics successfully control secondary hyperparathyroidism in patients with CKD and concomitantly lower serum levels of both calcium and phosphate. The administration of cinacalcet permits the suppression of PTH in patients not adequately controlled with vitamin D analogs, as well as the optimal control of PTH.28 Because of this improved biochemical control (i.e., reduced PTH without increased Ca × P), the possibility exists that the use of cinacalcet may reduce vascular calcifications and improve cardiovascular outcomes. Animal data and limited observational studies have suggested that cinacalcet may retard the progression of valvular, aortic and coronary calcification in dialysis patients.29
- Renal transplantation appeared to markedly slow down or abolish the progression of coronary artery calcification/vascular calcification in a small study.30 However, there are also reports on progressive calcification after transplantation.31
- Parathyroidectomy: There are only occasional reports on a beneficial role of subtotal parathyroidectomy.32
- Hyperbaric oxygen therapy has been shown to improve skin lesions in patients with distal forms of vascular calcification.33
- Sodium thiosulfate: This sequesters calcium ions to form highly soluble calcium thiosulfate complexes and can prevent calcium phosphate precipitation.34
OUR EXPERIENCE
At our center, we screened pre-ESRD (end-stage renal disease) [CKD stage 4 and 5] patients for the presence of vascular calcification using digital X-ray lumbar spine and multislice CT scan (Fig. 4). The prevalence of vascular calcification (abdominal aortic calcification) in pre-ESRD patients was 75% (73.6% and 81.8% for CKD stages 4 and 5, respectively). The median aortic calcification index was 19.9% in all patients, 18.5% in CKD stage 4 and 21.4% in CKD stage 5. Decreased glomerular filtration rate may be associated with the presence and extension of abdominal aortic calcification in pre-dialysis CKD stages 4 and5.35
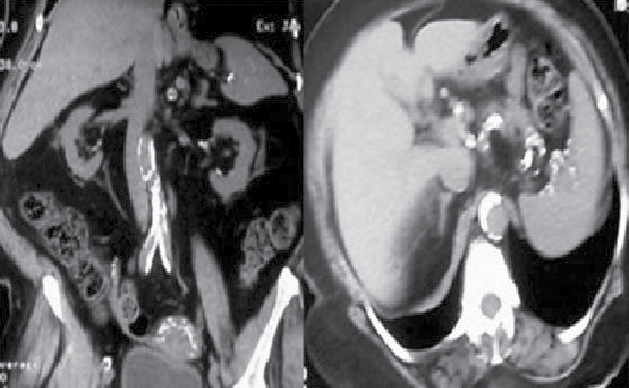
Figure 4. Multislice computed tomography image of abdominal aorta showing multiple calcification sites.
Funding source: Nil.
Acknowledgment: We acknowledge that Figure 2 was prepared online using platform provided by Biorender.com.
REFERENCES
- Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, et al. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med. 2000;342(20):1478-83.
- London GM, Guérin AP, Marchais SJ, Métivier F, Pannier B, Adda H. Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18(9):1731-40.
- Matsuoka M, Iseki K, Tamashiro M, Fujimoto N, Higa N, Touma T, et al. Impact of high coronary artery calcification score (CACS) on survival in patients on chronic hemodialysis. Clin Exp Nephrol. 2004;8(1):54-8.
- Goldsmith DJ, Covic A, Sambrook PA, Ackrill P. Vascular calcification in long-term haemodialysis patients in a single unit: a retrospective analysis. Nephron. 1997;77(1):37-43.
- Floege J, Ketteler M. Vascular calcification in patients with end stage renal disease. Nephrol Dial Transplant. 2004;19 Suppl 5:V59-66.
- Eifinger F, Wahn F, Querfeld U, Pollok M, Gevargez A, Kriener P, et al. Coronary artery calcifications in children and young adults treated with renal replacement therapy. Nephrol Dial Transplant. 2000;15(11):1892-4.
- Mohler ER 3rd. Vascular calcification: good, bad or ugly? Vasc Med. 2002;7(3):161-2.
- Shroff RC, Shanahan CM. The vascular biology of calcification. Semin Dial. 2007;20(2):103-9.
- O’Neill WC. The fallacy of the calcium-phosphorus product. Kidney Int. 2007;72(7): 792-6.
- Lockhart ME, Robbin ML, McNamara MM, Allon M. Association of pelvic arterial calcification with arteriovenous thigh graft failure in haemodialysis patients. Nephrol Dial Transplant. 2004;19(10):2564-9.
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009;(113):S1-130.
- Moshage W, Achenbach S, Daniel WG. Novel approaches to the non-invasive diagnosis of coronary-artery disease. Nephrol Dial Transplant. 2001;16:21-8.
- Moe SM, Chen NX. Pathophysiology of vascular calcification in chronic kidney disease. Circ Res. 2004;95(6):560-7.
- Mizobuchi M, Towler D, Slatopolsky E. Vascular calcification: the killer of patients with chronic kidney disease. J Am Soc Nephrol. 2009;20(7):1453-64.
- Franceschi RT, Xiao G. Regulation of the osteoblast-specific transcription factor, Runx2: responsiveness to multiple signal transduction pathways. J Cell Biochem. 2003;88(3):446-54.
- Chen NX, O’Neill KD, Chen X, Duan D, Wang E, Sturek MS, et al. Fetuin-A uptake in bovine vascular smooth muscle cells is calcium dependent and mediated by annexins. Am J Physiol Renal Physiol. 2007;292(2):F599-606.
- Levey AS, Beto JA, Coronado BE, Eknoyan G, Foley RN, Kasiske BL, et al. Controlling the epidemic of cardiovascular disease in chronic renal disease: what do we know? What do we need to learn? Where do we go from here? National Kidney Foundation Task Force on Cardiovascular Disease. Am J Kidney Dis. 1998;32(5):853-906.
- Chertow GM, Burke SK, Raggi P; Treat to Goal Working Group. Sevelamer attenuates the progression of coronary and aortic calcification in hemodialysis patients. Kidney Int. 2002;62(1):245-52.
- LeGeros RZ, Contiguglia SR, Alfrey AC. Pathological calcifications associated with uremia. Calcif Tissue Res. 1973;13(3):173-85.
- Watson KE, Abrolat ML, Malone LL, Hoeg JM, Doherty T, Detrano R, et al. Active serum vitamin D levels are inversely correlated with coronary calcification. Circulation. 1997;96(6):1755-60.
- Drissi H, Pouliot A, Koolloos C, Stein JL, Lian JB, Stein GS, et al. 1,25-(OH)2-vitamin D3 suppresses the bone-related Runx2/Cbfa1 gene promoter. Exp Cell Res. 2002;274(2):323-33.
- Nitta K, Ishizuka T, Horita S, Hayashi T, Ajiro A, Uchida K, et al. Soluble osteopontin and vascular calcification in haemodialysis patients. Nephron. 2001;89(4):455-8.
- Schafer C, Heiss A, Schwarz A, Westenfeld R, Ketteler M, Floege J, et al. The serum protein alpha 2-Heremans-Schmid glycoprotein/fetuin-A is a systemically acting inhibitor of ectopic calcification. J Clin Invest. 2003;112(3):357-66.
- K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45(4 Suppl 3):S1-153.
- Block GA, Spiegel DM, Ehrlich J, Mehta R, Lindbergh J, Dreisbach A, et al. Effects of sevelamer and calcium on coronary artery calcification in patients new to hemodialysis. Kidney Int. 2005;68(4):1815-24.
- Silver J. The details bedevil DCOR. Kidney Int. 2007;72(9):1041-3.
- Rosenblum IY, Black HE, Ferrell JF. The effects of various diphosphonates on a rat model of cardiac calciphylaxis. Calcif Tissue Res. 1977; 23(2):151-9.
- Block GA, Martin KJ, de Francisco AL, Turner SA, Avram MM, Suranyi MG, et al. Cinacalcet for secondary hyperparathyroidism in patients receiving hemodialysis. N Engl J Med. 2004;350(15):1516-25.
- Aladrén Regidor MJ. Cinacalcet reduces vascular and soft tissue calcification in secondary hyperparathyroidism (SHPT) in hemodialysis patients. Clin Nephrol. 2009;71(2):207-13.
- Moe SM, O’Neill KD, Reslerova M, Fineberg N, Persohn S, Meyer CA. Natural history of vascular calcification in dialysis and transplant patients. Nephrol Dial Transplant. 2004;19(9):2387-93.
- Schankel K, Robinson J, Bloom RD, Guerra C, Rader D, Joffe M, et al. Determinants of coronary artery calcification progression in renal transplant recipients. Am J Transplant. 2007;7(9):2158-64.
- Bleyer AJ, Burkart J, Piazza M, Russell G, Rohr M, Carr JJ. Changes in cardiovascular calcification after parathyroidectomy in patients with ESRD. Am J Kidney Dis. 2005;46(3):464-9.
- Rogers NM, Chang SH, Teubner DJ, Coates PT. Hyperbaric oxygen as effective adjuvant therapy in the treatmentof distal calcific uraemic arteriolopathy. NDT Plus. 2008;1(4):244-9.
- Schlieper G, Brandenburg V, Ketteler M, Floege J. Sodium thiosulfate in the treatment of calcific uremic arteriolopathy. Nat Rev Nephrol. 2009;5(9):539-43.
- Himanshu, Sunder S, Venkataramanan K. Screening for the prevalence of vascular calcification in pre-ESRD (CKD Stage 4 &5) Indian patients – A single center experience. Abstract, Asian Forum of CKD and Indian Society of Nephrology, Northern Chapter, Annual Meeting, Chandigarh 2012.
|